
| John Baker, our Managing Partner, has researched two railway accidents that happened at the same Somerset village 50 years apart. This research has been in support of Norton Fitzwarren's bid to receive a 'red wheel' heritage plaque from the Transport Trust in recognition of the villagers' efforts to rescue the victims in both crashes. The leader of the project, Mary Hayward, had seen our news article on the 1940 accident and asked if we could help with her research. Of course, we were delighted to help especially since both accidents had a significant 'human factor' element. We have previously written a short article on the 1940 accident, but the accident of the 11th November 1890 was also blamed on 'human error'. In this accident the signaller, George Rice, forgot that he had left a goods train standing on the main line and allowed an approaching fast passenger train into the same section. The passenger train collided with the stationary goods engine, killing 10 passengers and seriously injuring many more. John's research revealed several new facts about both accidents and also documented more about the victims and those involved. This research has been published on posters that will be displayed in Norton Fitzwarren Village Hall. Copies of the posters for download are included at the end of this article. As part of the Red Wheel project, John was asked to give a radio interview to the BBC - this is now available on the BBC website. On the 17th November, the Transport Trust awarded Norton Fitzwarren with a 'Transport Heritage Site' award. We were delighted to attend to see the culmination of Mary Hayward's work to get the actions of the villagers recognised following these two tragic accidents.
|  Transport Heritage Site award 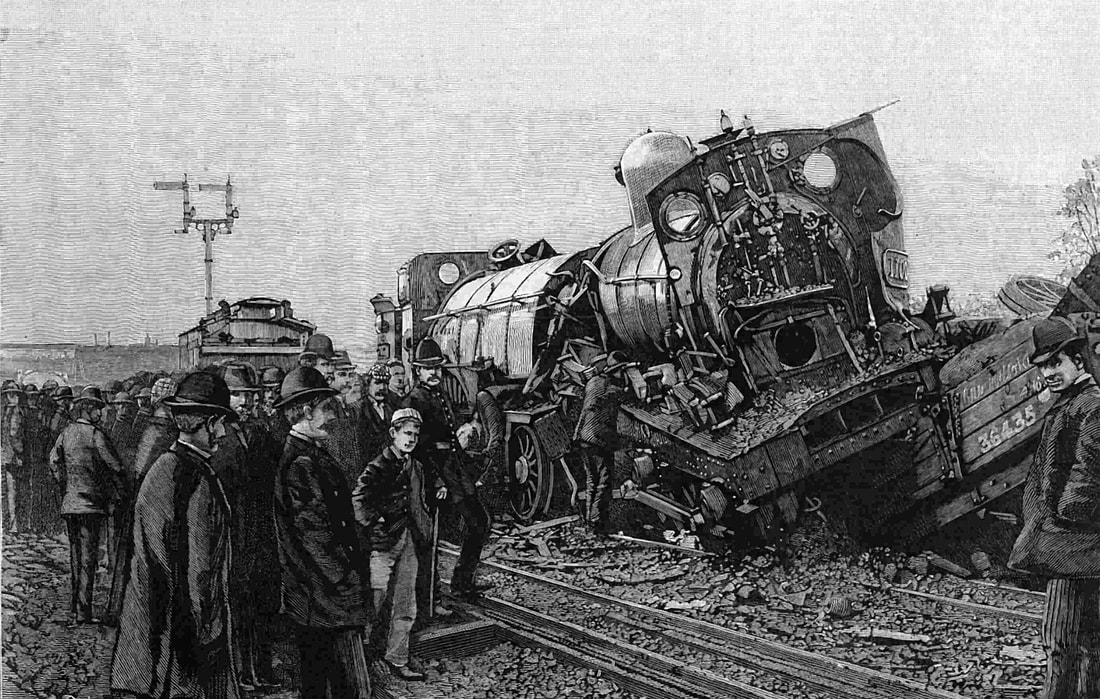 Locomotives in the 1890 accident 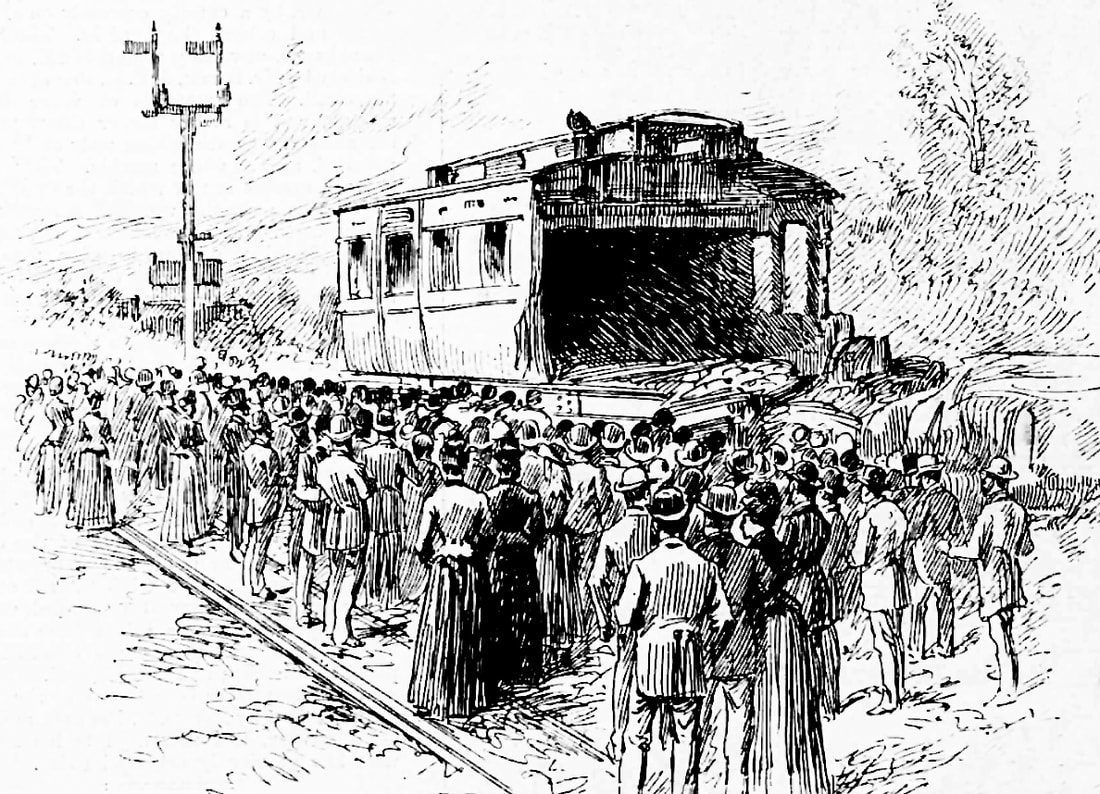 Damaged coach in the 1890 accident 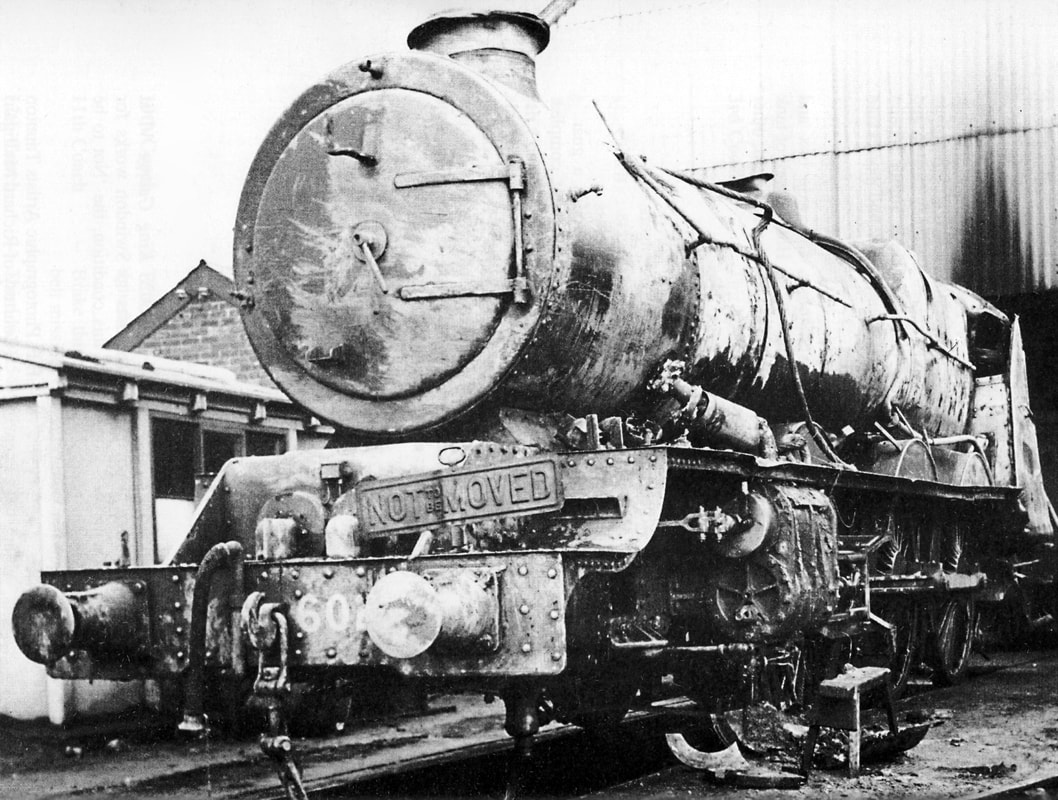 Locomotive after recovery in 1940 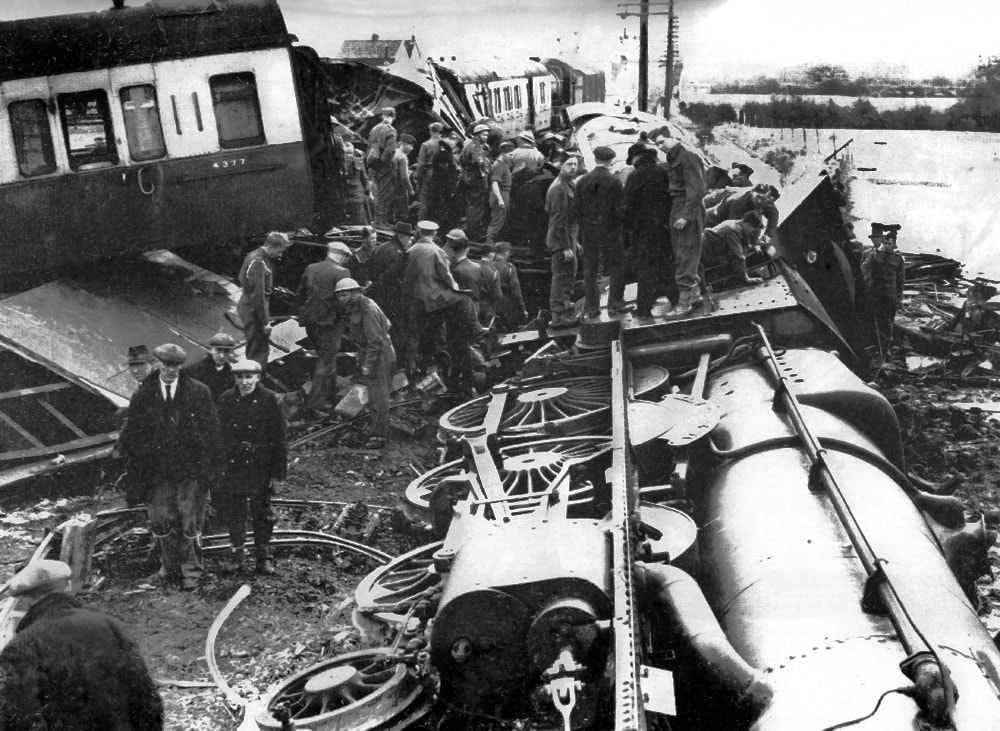 1940 accident site  Site of the 1940 accident | ||||||||||
|
1 Comment
 Photo: KentOnline Photo: KentOnline Human errors often have humorous rather than safety critical consequences. The two examples here illustrate system failures which caused embarrassment for the organisations involved, but probably nothing more. In the top example, a sub-contractor working on street repairs after gas main works made the road marking error. Instead of marking the temporary space as 'DISABLED', a rather different marking was made. The operator was probably doing the best they could - the real failure is in the system that allowed the error to occur. See the KentOnline news report for the full story.  Photo: BT.com Photo: BT.com In this second example, road painters repeated a spelling error that was first introduced on the section of road two years previously. Here, 'MINUTES' was replaced with 'MINUITES'. Again, the error lies in the system somewhere, not with the individual carrying out the marking. For the full story, see BT.com.
 Research by the International Atomic Energy Authority (IAEA) published in December 2013 showed that 80% of significant events at nuclear power plants can be attributed to human error, while only 20% can be attributed to equipment failure.
For many years the belief has been that human error is an individual-focused phenomenon or motivational issue. However, it has recently been identified that approximately 70% of these errors are down to weaknesses in organisational processes and cultural values. These organisational deficiencies are often hidden in management processes, structures and values and can create workplace conditions that lead to a human error or reduce the effectiveness of risk control barriers. The full report can be viewed here. See our pages on how we help organisations manage the conditions that can lead to errors and our accident investigation pages. |
Archives
November 2020
Categories
All
|





 RSS Feed
RSS Feed