
| John Baker, our Managing Partner, has researched two railway accidents that happened at the same Somerset village 50 years apart. This research has been in support of Norton Fitzwarren's bid to receive a 'red wheel' heritage plaque from the Transport Trust in recognition of the villagers' efforts to rescue the victims in both crashes. The leader of the project, Mary Hayward, had seen our news article on the 1940 accident and asked if we could help with her research. Of course, we were delighted to help especially since both accidents had a significant 'human factor' element. We have previously written a short article on the 1940 accident, but the accident of the 11th November 1890 was also blamed on 'human error'. In this accident the signaller, George Rice, forgot that he had left a goods train standing on the main line and allowed an approaching fast passenger train into the same section. The passenger train collided with the stationary goods engine, killing 10 passengers and seriously injuring many more. John's research revealed several new facts about both accidents and also documented more about the victims and those involved. This research has been published on posters that will be displayed in Norton Fitzwarren Village Hall. Copies of the posters for download are included at the end of this article. As part of the Red Wheel project, John was asked to give a radio interview to the BBC - this is now available on the BBC website. On the 17th November, the Transport Trust awarded Norton Fitzwarren with a 'Transport Heritage Site' award. We were delighted to attend to see the culmination of Mary Hayward's work to get the actions of the villagers recognised following these two tragic accidents.
|  Transport Heritage Site award 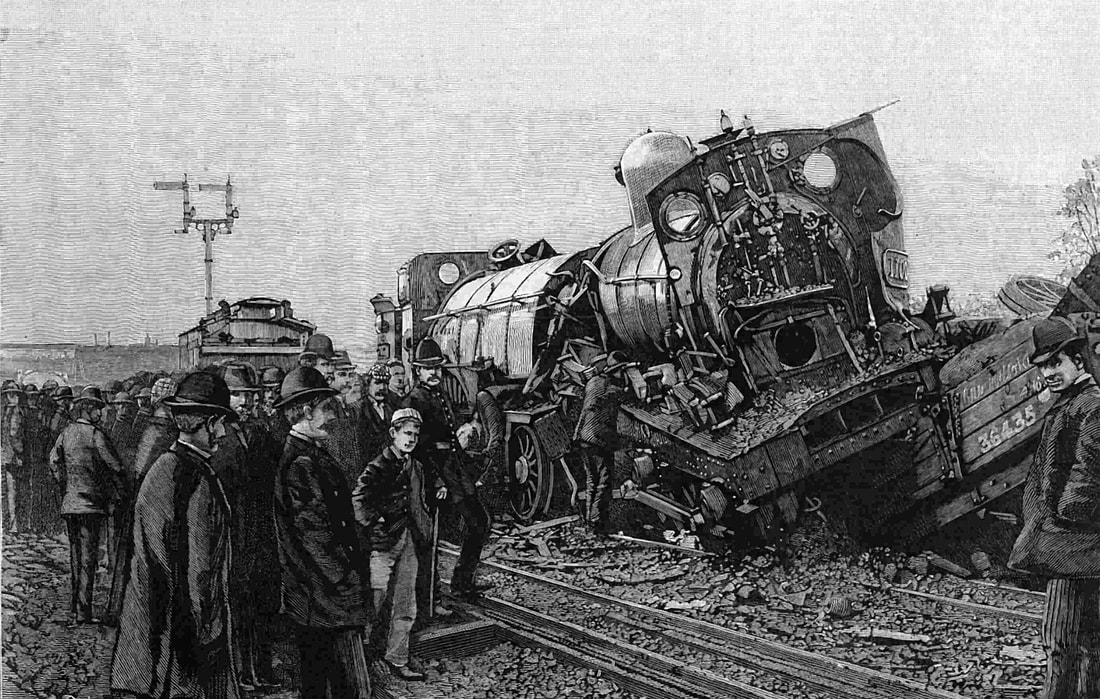 Locomotives in the 1890 accident 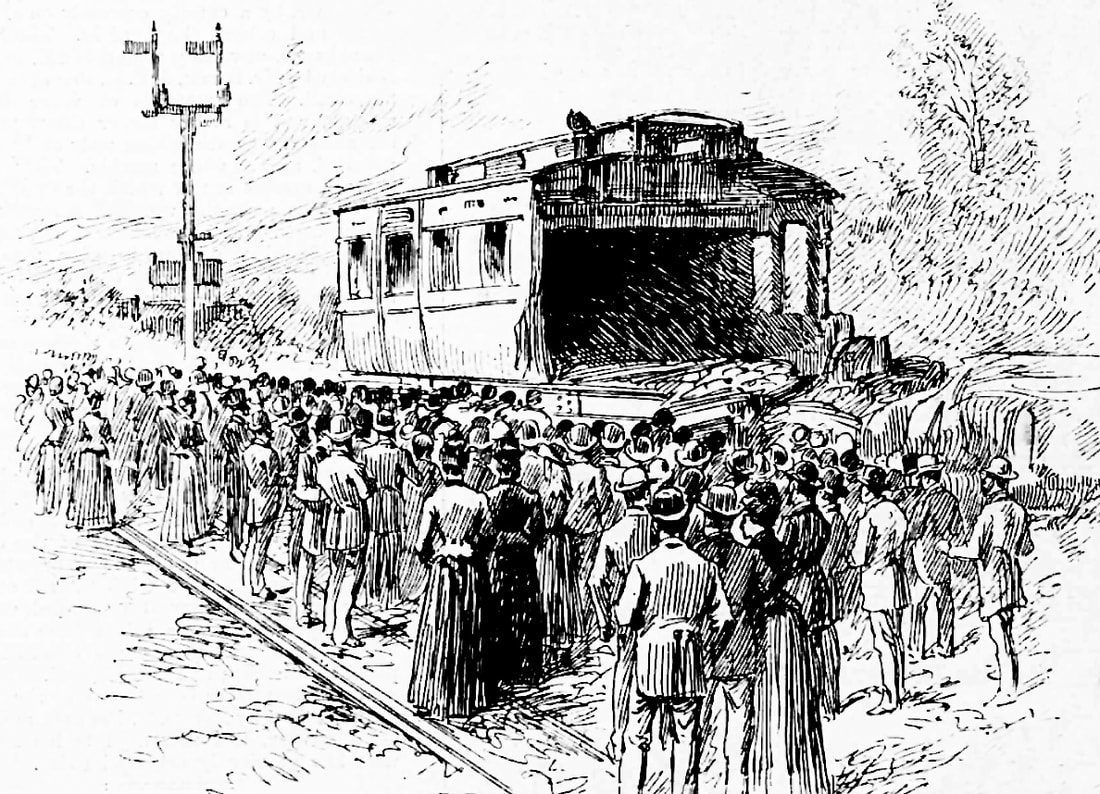 Damaged coach in the 1890 accident 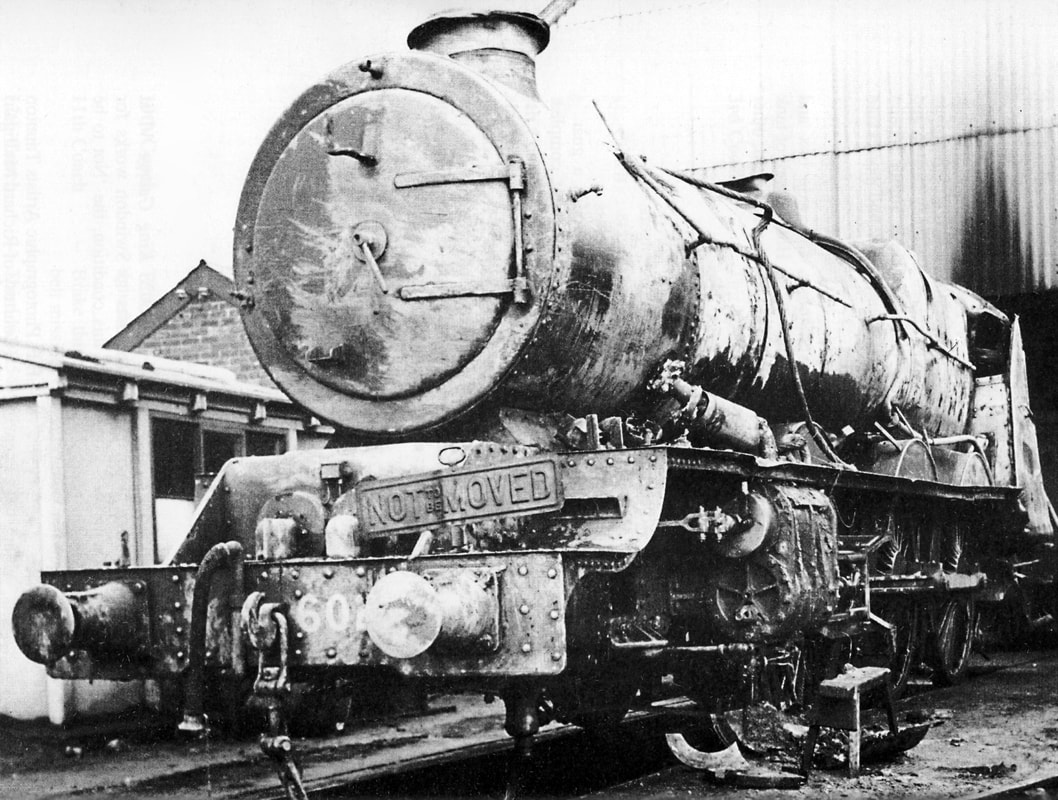 Locomotive after recovery in 1940 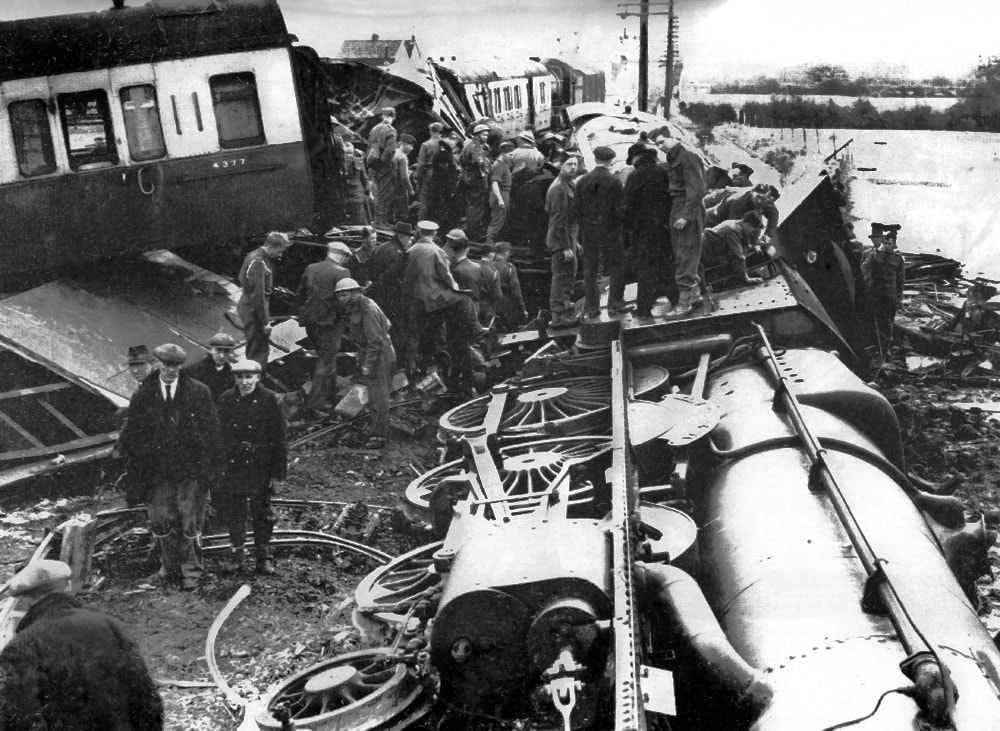 1940 accident site  Site of the 1940 accident | ||||||||||
|
1 Comment
On the 12th December 1988 a crowded passenger train crashed into the rear of another train that had stopped at a signal, and an empty train, travelling in the other direction, crashed into the debris. Thirty-five people died and nearly five hundred were injured.
The primary cause of the crash was incorrect wiring work on the signalling system; a redundant wire was left connected at one end, and bare at the other. The wire came into contact with a relay, causing a signal to display a 'wrong side' green aspect regardless of the presence of a train on the track circuit. The signalling technician responsible had also worked a seven day week for the previous thirteen weeks. Twenty five years on from the Clapham Junction rail disaster, a survivor is still remembering fresh details from that harrowing day. See the news item here, and the accident report on the Railways Archive website here. WASHINGTON -- The NTSB continues to rule out mechanical causes in a deadly Bronx train crash while adding to the possibility that human error was involved. Federal safety investigators have all but eliminated mechanical problems as the cause of the December 1 derailment, but there are indications that the driver might not have been as attentive as he should have been.
See the news item here and the NTSB's page on this accident here. |
Archives
November 2020
Categories
All
|





 RSS Feed
RSS Feed