
Event recorders, often referred to as 'black boxes', have been common in the aviation and rail sectors for many years. These devices record critical actions of the operator (pilot or driver) as well as information about the vehicle such as speed and acceleration rates. Event recorders are mainly known for their use in reconstructing the events before a serious accident, but they can also be used proactively to unobtrusively monitor an operator's performance. Used in this way they can provide an opportunity to develop competence or change behaviour before an undesirable event occurs. We make use of event recorders in both competence management systems and during accident investigations for rail and tram clients.
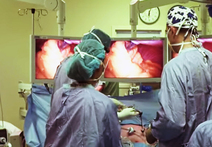
Now, a surgeon in Toronto is pioneering the use of these devices in surgery to help identify problems in preparation for surgery, and as a tool to investigate problems after they have happened. Read the full news story on the Toronto City News website.
Now, a surgeon in Toronto is pioneering the use of these devices in surgery to help identify problems in preparation for surgery, and as a tool to investigate problems after they have happened. Read the full news story on the Toronto City News website.





 RSS Feed
RSS Feed